Modified Radical Mastectomy
Simultaneous removal of the mammary gland, subject to fascia, subscapular, axillary 1-2-level and intermuscular tissue with lymph nodes.
<20
minutes
Preparation
40-120
minutes
Operation time
3-5
days
period
Complexity:
Средняя
Type of anesthesia:
ETA/mask anesthesia
Diagnostic minimum:
- Anamnesis
- Physical examination of mammary glands
- Mammography
- Ultrasound of mammary glands and regional lymph nodes
- Trepan-biopsy of mammary gland formation
- Histological and immunohistochemical examination of tumor tissue
- Ultrasound of the abdominal cavity organs
- Ultrasound of the pelvic organs
- Rg of the thorax
- Osteoscintigraphy (with locally distributed variant)
- Clinical blood test
- Blood chemistry
Preoperative preparation:
Position of the patient on the table:
- On the back in a horizontal position with a withdrawn arm on the side of the operation
Location of the operating team:
Video operations:
Technique of operation: Step 1.
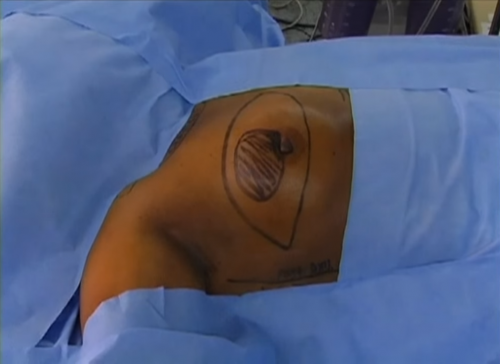
After preparing the surgical field, the surgeon marks two horizontal semi-oval lines bordering the mammary gland.

After the marking, it cuts them with a scalpel to the deep layers of the dermis and cuts the surgical coagulant to the subcutaneous fat while coagulating the small bleeding vessels.
After the marking, it cuts them with a scalpel to the deep layers of the dermis and cuts the surgical coagulant to the subcutaneous fat while coagulating the small bleeding vessels.
Technique of operation: Step 2.
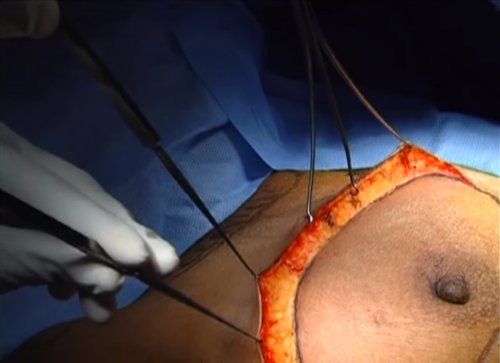
Mobilization of skin flaps. To do this, the assistant takes the edges of the flaps on the sharp one-tooth hooks of the Chassignac (can be taken on the holders) and rearranges them as the flaps are mobilized, the operator in the meantime mobilizes the skin with the adjacent fiber with a surgical coagulant right down to the large pectoral muscle forming the upper and lower flaps.
The mammary gland remains fixed to the large pectoral muscle in the fatty capsule.
The mammary gland remains fixed to the large pectoral muscle in the fatty capsule.
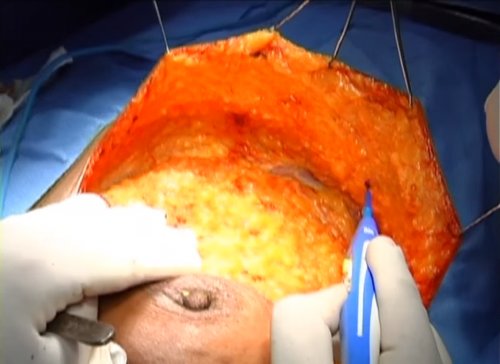
Technique of operation: Step 3.
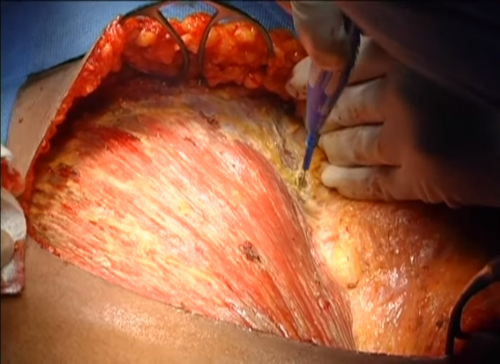
With the help of a surgical coagulator, the mammary gland is separated from the large thoracic, jagged muscle from the medial edge of the breast and laterally up to the axillary region.
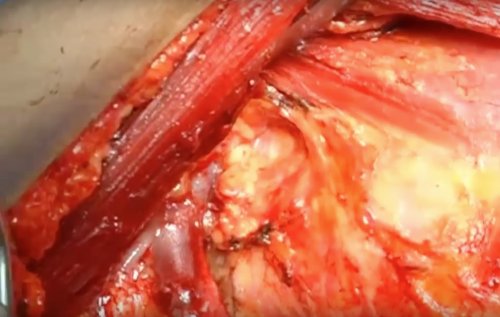
Technique of operation: Step 4.
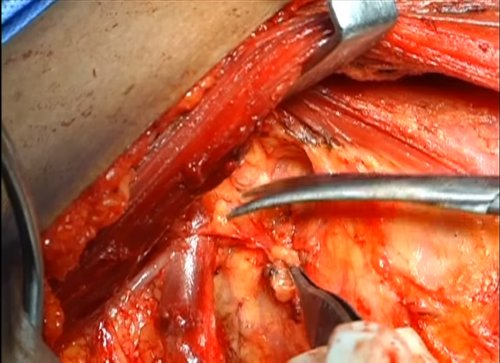
When working in the axillary region, light is created for a better view, the power of the coagulator is reduced for more delicate work with the tissues. Mobilizing the axillary tissue near the axillary - subclavian vein should not use a coagulator in order not to damage large vessels, the most convenient in this case surgical scissors for Cooper with curved ends. The assistant in the meantime lifts the edge of the large pectoral muscle with a four-tooth blunt hook or a hook of Farabef. The surgeon has scissors parallel to the main vessels (axillary artery and vein) and in small steps the axillary fiber is separated from the axillary and subclavian veins reaching the inner edge of the small pectoral muscle. Large vessels that depart directly from the main ones are sent to the removed cellulose and the mammary gland are taken to the Moscow clamp, intersect and are bandaged with capron. In the deeper layers of the axillary tissue, a thoraco-dorsal vascular-neural bundle is distinguished along the anterior surface of the latissimus muscle of the back, a long thoracic nerve is also inside it, which serves as the medial border of lymphodissection. Having selected the basic anatomical structures of the axillary region, the axillary tissue is separated from the anterior surface of the latissimus muscle of the back. Thus, the mammary gland is removed in a single block with axillary tissue of I-II levels simultaneously with the implementation of hemostasis.
Technique of operation: Step 5.
The audit of the operating field, control hemostasis is performed.
Technique of operation: Step 6.
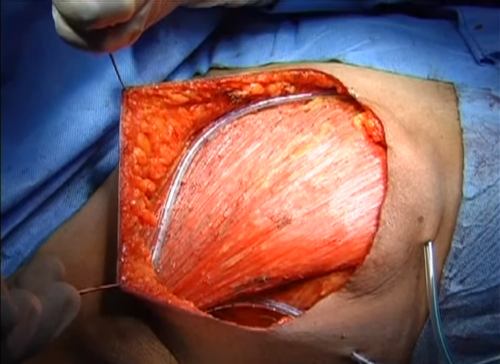
Installation of drains - one in the armpit, the other under the flaps.
Technique of operation: Step 7.

The wound is sutured by the vikril on the atraumatic needle 3/0 from the medial end of the wound to the lateral. If there is a strong tension of skin flaps, then it can be sewn in two rows, again with the vickry-3/0 first row and the PDS second.
Re-treat the skin in the area of the seams and apply aseptic dressings.
Postoperative period:
- Pharmacotherapy
- Bed rest
- Restriction of physical activity
Typical errors:
- Incorrect marking of the incision - tissue deficit - excessive tension of the edges of the wound
- Non-compliance with the rules of the oncological operation (a cut near the edge of the tumor)
- Too thin or thick grafts
- Erroneous ligation of thoraco-dorsal vein
- Axillary vein injury
- Separate removal of the mammary gland and axillary tissue (especially in lean cells)
Автор: Tsyvanenko Vadim Yurievich
Освоить навык можно на курсах:
Document Tags:
#,
Found an error in the text? Select it and press +
Instruments
Access
- Skin-liners
- Marker for marking
- Scalpel
- Surgical coagulator
- Sharp one-tooth hook Chassenyaka (2x)
- Antiseptic solution
Operative reception
- Surgical coagulator
- Hook with four-toothed blunt / hook of Farabef
- Cooper surgical curved scissors
- Non-resorbable sutures (capron)
- Surgical scissors blunt-pointed straight
- Surgical forceps
- The Moscow clamp
Exiting the operation
- Ulmer drainage catheter with a trocar
- Needle Holder Geghar
- Vicril with atraumatic needle 3/0
- Surgical scissors blunt-pointed straight
- Antiseptic solution