Laparocenesis. Operation technique.
Treatment-diagnostic surgical manipulation, the purpose of which is to detect damage to internal organs, remove effusion, administer drugs.
20-30
minutes
Preparation
20-60
minutes
Operation time
2-3
days
period
Complexity:
Низкая
Type of anesthesia:
Local anesthesia
Preoperative preparation:
Position of the patient on the table:
- Sitting with his feet down with a support arm
- Lying on the back
Location of the operating team:
Video operations:
Technique of operation: Step 1.
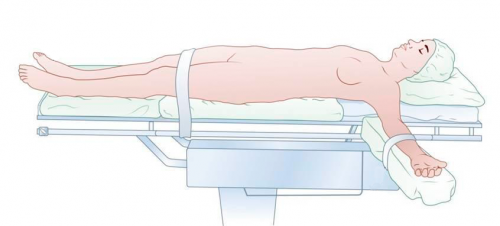
Help the patient to take the right position (sitting with his legs down with a support for the arms and back or in a serious condition lying on his back).
Technique of operation: Step 2.
Wash your hands and put on gloves.
Technique of operation: Step 3.

Treat the skin (alcohol, iodine).
Technique of operation: Step 4.

At the puncture site (usually along the middle line 2 cm below the navel, it is also possible to determine the puncture point by ultrasound of the abdominal cavity) perform an infiltration anesthesia with 0.25-0.5% solution of novocaine or with a 0.5-1% solution of lidocaine up to the peritoneum.
Technique of operation: Step 5.

Using a pointed scalpel, make a cut (5-10 mm) of the skin, subcutaneous tissue and aponeurosis (with a weakly expressed subcutaneous fatty tissue).
Technique of operation: Step 6.

Take the trocar or puncture needle into the leading arm, with the index finger of the second hand, take the cannula of the trocar or the puncture needle at a distance from the end corresponding to the estimated thickness of the anterior abdominal wall.
Puncture direction strictly perpendicular to the skin surface
Technique of operation: Step 7.

Slowly but decisively, rotate the peritoneal wall with pivotal movements (the moment of entering the abdominal cavity - the sensation of a sudden cessation of resistance, is also described as a feeling of "failure").
Technique of operation: Step 8.

Fixing the cannula with the finger of the left hand, the right one, quickly remove the stylet, while the ascitic fluid begins to flow freely into the previously substituted container.
Technique of operation: Step 9.

To the prospective place of fluid accumulation through the trocar sleeve, extend the rubber or polyvinylchloride tube with the side holes - the "balling" catheter and aspirate the contents of the abdominal cavity.
If you use a puncture needle - after receiving fluid from its lumen, attach a tube to connect the needle to the collection tank.
Technique of operation: Step 10.

Release fluid from the abdominal cavity slowly (about 1 liter for 5 minutes).
Technique of operation: Step 11.

After removing the liquid, remove the trocar, apply a septic patch over the skin at the puncture site. The tube can be left as a control drainage (diagnostic puncture) or to control and evacuate the accumulated fluid (therapeutic puncture), fixing it to the skin with a ligature (silk, kapron).
Postoperative period:
- Restriction of physical activity
- Seams removal for 7 days
Typical errors:
- Before conducting anesthesia, the patient should clarify that he has an allergy to anesthetics.
- The puncture of the abdominal wall should be carried out away from the post-operative scars, because they may have collateral vessels and adhesions to the intestinal tract.
- Release the liquid slowly (1 liter for 5 minutes), for this purpose a rubber clamp is periodically applied to the rubber tube. From time to time, the flow of intra-abdominal fluid should be interrupted for 2 to 4 minutes. If the fluid flow spontaneously stops, you can change the position of the cannula by tilting it in one direction or the other and slightly pushing it deeper.
- When the tube is left (step 11/11), the patient should be advised periodically to change the position in the bed to evacuate more fluid.
- After the infiltration anesthesia to the peritoneum, the ascitic fluid can be dialed into the syringe without much effort, but with a large thickness of the abdominal wall, the length of the injection needle may not be sufficient.
- If necessary, the fluid is taken for the study (the main tests include a cytological study, bacteriological culture, determination of the concentration of albumin and the total protein, amylase)
Освоить навык можно на курсах:
Document Tags:
#,
Found an error in the text? Select it and press +
Instruments:
Access
- Scalpel, blade 11/21
- Needle Holder Geghar
- Needle cutting 3/8 40-50mm for leather
- Suture material (silk, capron)
- Alcohol solution of iodine
- Medical alcohol
Operative reception
- Troakar or fat puncture needle with mandrel
- Drainage tube with side openings
- The most convenient and safe are special abdominal trocars with a protective flap and a side crane
- Tweezers, anatomical, surgical
- Clamp
- Anesthetic solution (novocaine 0.25-0.5% or 0.5-1% lidocaine solution)
Exiting the operation
- Syringe 10-20 ml with injection needle
- Tank for collection of liquid